Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Suicide has been a part of society and has lasting effects on many individuals. It is sometimes supported, but usually condemned. Some people argue that we have a right to die, as an extension on our rights of freedom of speech and freedom of thought. Globally suicide is already the highest in people older than 70. Euthanasia and physician-assisted suicide have become pressing public issues that are not typically discussed, even though it affects the lives and families of many. There are many questions that are raised without answers, such as who should be eligible for physician assisted suicide? Doctors are supposed to save lives. But what if no matter of medical intervention can help change someone’s imminent death? Should doctors then be allowed to help patients die on their own terms? If you allow physician assisted suicide, how close are we to condoning mass physician assisted suicide – what is now known as the Holocaust? Is this a “slippery slope”?
According to the Hippocratic Oath, assisted suicide would be outside of a physician’s professional responsibilities (Jr., W. C. S. ,2018). The five principles of bioethics include autonomy, justice, beneficence, non-maleficence, and fidelity and are each said to be absolute truths in and of themselves. However, beneficence, the prevention of harm or the doing of good, conflicts with respect for autonomy when one considers assisted suicide.
When interviewing Bonnie Hafeman M.D., a family physician with a subspecialty in Hospice and Palliative Care, who has worked in Hospice for 23 years, she said “I think that physician assisted suicide is totally unnecessary because people are given all of the tools they need to control their own death. The easiest way to do so is just to not eat and drink. This is a relatively painless death that takes about a week. And it is natural.”
She states that “It is immoral to involve another human being in your own death because that is really between you and God. I think that when you do physician assisted suicide it is just a publicity stunt.”
I think that this has to do with how they present themselves and how they talk to others. It makes me wonder what kind of relationship they have with their physician. Physicians should be there to give advice and to help plan out where they want to go with their lives, but I don’t think it is right to have another person be responsible for their death. The increase in this event, and the legalization and acceptance of the physician assisted suicide may lead to the undesirable action which is involuntary euthanasia. Once one becomes common practice, society becomes used to something become a norm and it expand it until it reaches a nonlogical position. Once we allow voluntary euthanasia, we may fail to make the distinction and make the morally unacceptable use to use involuntary euthanasia.
Dr. Hafeman goes on to say, “The most commonly cited need for assisted suicide is the condition ALS where your body loses muscle function so you cannot swallow or move so you may end up being locked where you can still see and hear people, but not talk or interact with them. Those same people are also advised to have gastric tubes placed to feed them. If they weren’t being fed artificially they would die naturally by dehydration without ever being locked in. A person should have access to terminal pain control, and how they use this is often beyond the control of the physician who prescribed it. If a person does not have access to pain control the answer is not physician assisted suicide, it is giving the person adequate pain control. Yes, this might hasten a patient’s death. However, it is a balance between intention to commit suicide and a patient’s right to have pain controlled.”
Even though one may wish to alleviate suffering, assisting with death to end the suffering violates the principle of beneficence even though the individual may in autonomy, request death.
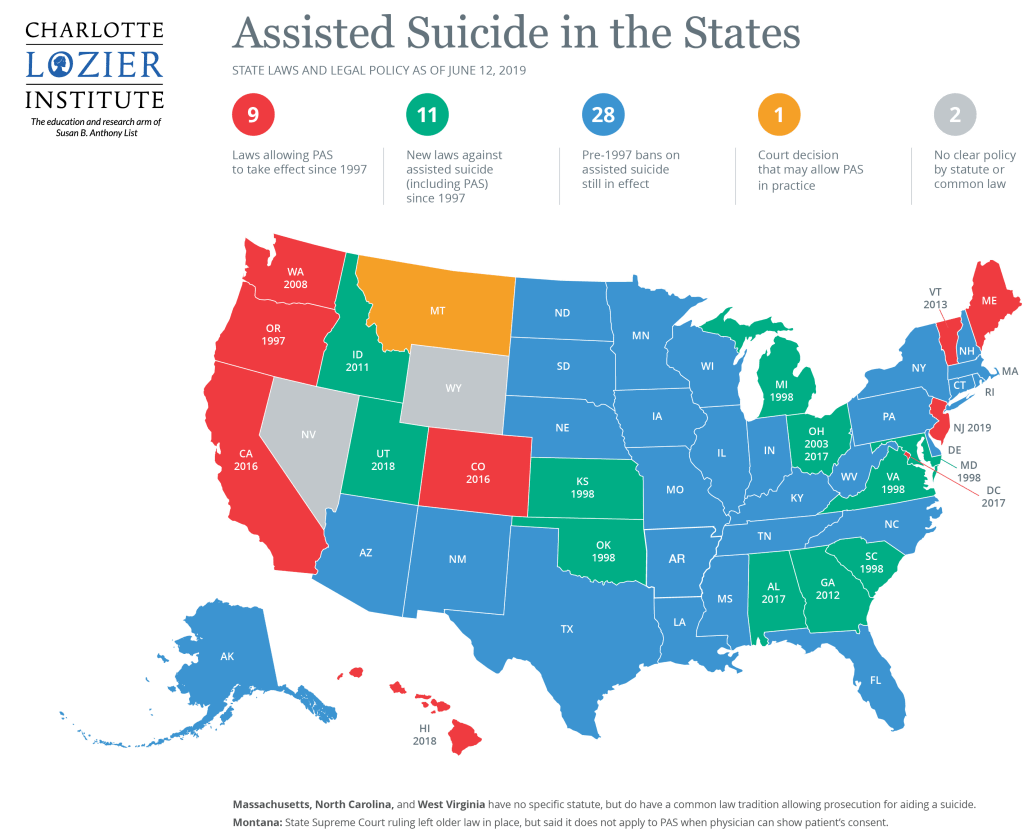
In many states, physician assisted suicide (PAS) has been deemed as a socially acceptable way to end a life if there is extreme suffering. As you can see in the figure below, today, it is legal in 10 jurisdictions as of January 2020, with Oregon being the first when they enacted their Dignity Act in 1997.
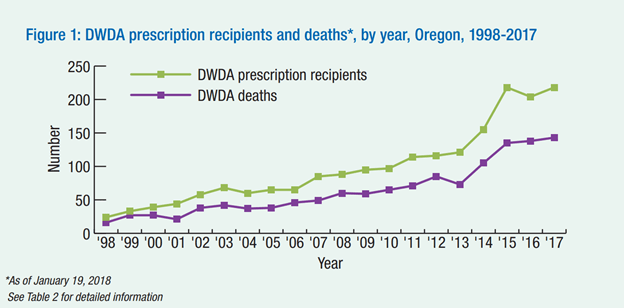
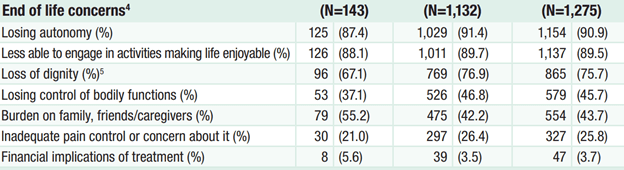
In the figure shown below, you can see that in Oregon, there has been an increase in physician assisted suicides and an even higher increase in requests since it became legal in 1997. These numbers are rising. This act is done by ingesting a lethal medicine dose prescribed by them after the request. The Oregon Death with Dignity act 2017 Data Summary shows that most patients request that request assisted suicide at 88.1% is because they cannot participate in activities making life enjoyable. 87.4% choose to over lose autonomy and 61.7% choose to because of dignity. They give validating reasons for why they choose to go on with PAS. This can all be seen in the data table shown below.
As of right now, we are comfortable to allow PAS for people who are terminally ill and near the end of their life, but so far we have dragged our feet when it comes to expanding to those who can gain access to PAS in the United States.
In a survey by Dr. Emanuel done in 2002, he looks at the attitudes of the American publics, of physicians, and of patients. He found that in all three of the survey categories that people who were reported as religious were more likely to be opposed to euthanasia or PAS. This may have to do with the belief in life after death and that the time of suffering or death is a time of awareness or connection with God. It’s not the pain itself that’s an issue, but about the connection with God. African Americans and older individuals are also more opposed to PAS. This may have to do with their deep seeded religious beliefs. Some surveys showed women as more opposed. A reason for this is because they are primarly care takers. They can see beyond the pain. However, patients with terminal illnesses had attitudes that were almost identical to the public. Physicians also has similar attitudes, however were less supportive if they were more likely to be called to actually perform the act. This may explain why oncologists (as many PAS patients have cancer) are the least supportive of physicians. (Emanuel, 2002)
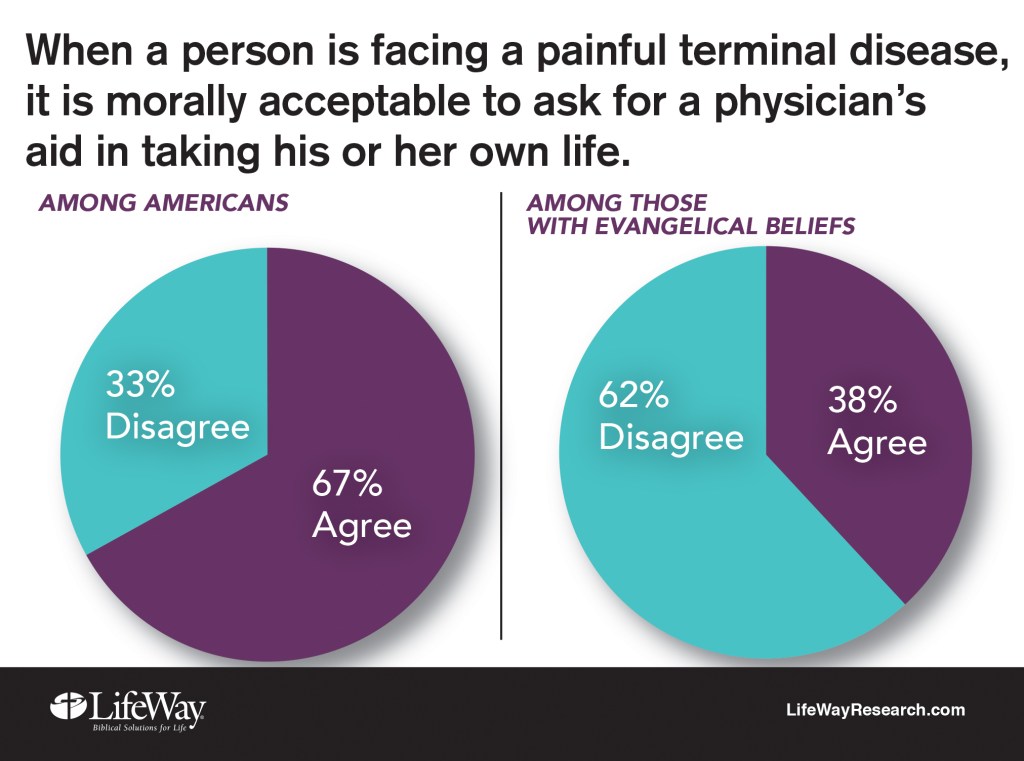
According to a survey from Nashville-based LifeWay Research, even though millions of Americans disagree with assisted suicide, the majority (about two-thirds of the population) say that it should be morally acceptable for terminally ill patients to have access to physician assisted suicide. Suffering up until death should not be the only out. This survey can be seen in the figure below.
So far, the United States has not expanded the criteria past the terminally ill. An issue is including those who are suffering from mental health illness. Society still highly stigmatizes mental health and it is a topic that most of the public knows very little about. Furthermore, mental illness can manifest very differently in individuals, but we use umbrella terms to categorize a wide variety of mental health symptoms. Because most people are not well versed in the scope of mental illness it leaves us hesitant to expand the criteria of people eligible to choose PAS. This is the slippery slope that can lead to condoning a sort of holocaust. It, along with people with physical disabilities, was one of the first excuses that were used by physicians in the Nazi Party.
Another reason we have not expanded the criteria is not because we think that no one else could be suffering as much as patients who are terminally ill, but because citizens and policy makers may be fearful that expanding the criteria for PAS would mean we’d have to allow patients to choose to die when we have the technology to heal them and extend their lives.
There are three distinctions of euthanasia. The first is active and passive euthanasia. (Abohaimed, et. al, 2019) Which, while there is a very distinct legal line between active and passive euthanasia, sometimes making that decision to “let a person die” seems to be an active decision. This is can be seen in a Munson’s reading of Baby Owens from of a child with Down Syndrome and duodenal atresia that was asked to not be treated (Munson, 2008, pp 630-631). While this is technically passively letting the child die, making the decision to not treat an easily treatable case doesn’t feel passive. It seems that extending a life that has the potential to be long and happy should be done.
The second distinction of euthanasia is voluntary and nonvoluntary euthanasia. (Abohaimed, et. al, 2019) While we aren’t actively euthanizing people against their will (that would never be considered an allowable practice) there is talk about full consent regarding euthanasia. We want to use euthanasia to ease a person’s suffering, but not if they feel forced to do it because of social pressures. An article from Callahan talks about a person to have the ability to choose to be euthanized if the suffering is great and their autonomy needs to be respected when they make that decision (Munson, 2008, pp 706-711). The article does not address some of the social reasons an individual may feel forced to choose euthanasia. For example, “Dead at Noon” is a suicide note where Gillian Bennett felt that she was a burden and that her continued existence would increase the suffering of her family (Bennett, 2014). This letter can be read at the following link.
Social pressures can cause someone to pursue euthanasia and having the option may send the message to other people with similar cases that they are living lives that are not worth living. On the other hand, what one person deems as a good life may seem unbearable by another. While I agree that we need to be doing more to alleviate the social pressures that individuals like Bennett felt, I think that we will never be able to overcome all of them and that working on easing the lives of individuals suffering from diseases and disabilities can happen at the same time that euthanasia is being practiced. We cannot take away someone’s ability to make an autonomous decision because things “might” get better. And we cannot use future research or outcomes to justify actions that are taken in the moment.
The third distinction between euthanasia cases is speeding up a death verses ending a life. (Abohaimed, et. al, 2019) This is a harder distinction to make but is relevant when we are making policies in regard to euthanasia since most places require that you are terminally ill. An example of this would be for a baby who has a disease where its skin is falling off… people may want to be able to end the baby’s life despite it being an active killing because the baby was in constant pain and was terminally ill. On the other hand, Munson’s book includes a boy named Dax who is not allowed to die because he was not terminally ill even though he was in great pain (Munson, 208, 98-101). There seems to be a balance between autonomy and a terminal illness that is hard to strike. I believe that PSA and euthanasia is more than just about the fact of autonomy, but much more complicated. To adequately allow people with extreme suffering to choose PAS, the criteria for eligibility must be expanded.
One solution is that eligibility for PAS should be available to those who have maxed out their treatment options for mental and physical ailments. PAS is meant to decrease suffering in patients who really have no hope left. This is not adequately covered with only the terminally ill. If we were to expand the criteria to apply for PAS to include people who have maxed out the treatment options available for either their physical illness or their mental illness we could be more true to the reasons we have wanted PAS to be available for people. Maxing out treatment is not an easy thing to do and will take most people several years, but if there is truly no treatment available for a patient and they feel that they are in enough suffering to want to apply for PAS then we can confidently say as a society that there is not anything we could medically do to help them. This would not allow someone that has not maxed out treatment to choose PAS. It would exclude many illnesses such as those in the forms of depression which may happen even in our youth as there are many treatment options that work for those cases. Expanding eligibility for PAS to include those who have maxed out their treatment options will not cover all the cases of extreme suffering, but it is a step towards it and prevents a lot of the slippery slope arguments that prevent the policy from being expanded.
Another solution that has been used in the past is to allow PAS to terminally ill patients but require a waiting period of just in case people change their mind. PAS in the united states currently takes up to six weeks as you need to go through the court process, see a psychiatrist, and have two physicians sign off on it before you are prescribed the lethal dose of medication. This makes it go over better in our society but adds a lot of unnecessary time for the patient that has made the decision already.
Another solution is not to allow PAS at all, but to have adequate pain control even at the risk of hastening a patient’s death. This allows a physician to still follow the five principles of bioethics as their intention is still to help their patient alleviate pain.
Another solution is for the patient to just commit suicide unassisted by the physician. Suicide is within the means of most people. I think that it is a choice that people must make. If you think that it’s going to be painful, then you lack imagination. I don’t believe it’s a moral choice to make, but it’s not my place to judge. I just don’t think you should put another person in that position.
I think that dying naturally teaches lessons. It teaches grace and is a time for communication that people can wrap up their lives and forgive or be forgiven. It is connected with our birth as I believe life is a circle and if you interrupt that circle you lose some of the essence of life. If you miss that time period, you miss one of the major life events that make us human. The debate over physician-assisted suicide is unlikely to go away and it raises troublesome questions. It requires continuous ethical monitoring because it allows a person to start justifying the taking of a life.
Bibliography
Abohaimed, S., Matar, B., Al-Shimali, H., Al-Thalji, K., Al-Othman, O., Zurba, Y., & Shah, N. (2019). Attitudes of Physicians towards Different Types of Euthanasia in Kuwait. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6598031/
Bennett, Gillian. (2014) Dead at Noon. Retrieved from http://www.deadatnoon.com/. Website.
Charlotte Lozier Institute. (n.d.). Map: Assisted Suicide in the States. Retrieved from https://lozierinstitute.org/map-assisted-suicide-in-the-states/
Emanuel, E. J. (2002, January 28). Euthanasia and Physician-Assisted Suicide. Retrieved from https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/214736
Guy, M., & Stern, T. A. (2006). The desire for death in the setting of terminal illness: a case discussion. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1764532/
Jr., W. C. S. (2018, March 6). Medical Definition of Hippocratic Oath. Retrieved from https://www.medicinenet.com/script/main/art.asp?articlekey=20909
Most Americans Say Assisted Suicide is Morally Acceptable. (2017, August 23). Retrieved from https://lifewayresearch.com/2016/12/06/most-americans-say-assisted-suicide-is-morally-acceptable/ Munson, Ronald. (2008) Intervention and Reflection: Basic Issues in Medical Ethics. 8th edition. Thomson Higher Education; Belmont, CA. pp 630-631 and 98-101. Print.
Physician Assisted Suicide. (n.d.). Retrieved from https://illinoisrighttolife.org/physician-assisted-suicide/
The bright yellow house on the corner of East Houghton Drive and Townsend Drive always stood out to me (as pictured below). I noticed it my first time at Michigan Tech. The colorful exterior and prime location always made me wonder what its purpose was.

It wasn’t until this semester that I decide to check it out. I built up the courage to do so after career fair as I was just in an environment where I was outside of my comfort zone, talking to new people. I decided to build upon that feeling. I embraced ambiguity and contacted the Canterbury house for information on some of their events. That night I went to one of their Wednesday night dinners, not knowing anyone there, or anything about it. That night I experienced something unlike anything else I have ever been to.
I was uncomfortable when I first walked in as I was an outsider to this group. At first, I tried to fit in by watching other’s actions and following them. At this point in time I had made no connections and didn’t even know what the purpose of the Canterbury house was. I realized that the quickest way to answer my growing questions would be to start interacting directly with everyone there. Once I sat down by someone an introduced myself, I quickly made a friendship and learned all about the Canterbury house through asking questions. One connection led to more as they began to integrate me into their group. I met people from all over the world. I met people from all different backgrounds. I met people that spoke different languages. I met people that didn’t even go to Michigan Tech. And all these people were working towards a common goal. At first, I thought of myself as an outsider, but by social interactions I discovered similarities between myself and the other people there.
The meal itself wasn’t anything like I expected. That night we had Seoul food. It was unlike anything I had tasted, but it was delicious. I found out that each week, the dinner is a food from a different culture to promote diversity and allow international students to share recipes. There was a lot more people at the event than I thought there would be and it was very informal. Everyone was sitting on the floors, back of chairs, at the table. This was very unusual to me. I followed suit and sat on the floor next to a group of people. This spot was also where I ate my dinner as they didn’t eat at the table, just wherever they found room. Whenever you were handed a plate you could begin eating as the food was hot and there was “no point in waiting till it gets cold”. This was also different to me because I was raised where you had to wait for everyone to get their food before you begin eating the meal. I didn’t like the feeling that I was eating while others were still waiting for food. I kept looking around to see how other people would react, but to them it was normal. Nobody seemed to mind the scattered mealtime or waiting for their food to arrive. The dinner was only an hour long, but I ended up staying much later, helping clean up, meeting more people, playing games, socializing, and learning about those that I had met that night. Throughout my life, I have come to value the conversations after a meal as people are often more open and share stories from their lives during this time.
In no time, I had learned that the Canterbury House is a resource for students at Michigan Tech provided through the Episcopal Church. However, it does not press their religious affiliation within the house. They don’t have anything religiously based at the house. Anyone is welcome there as it was established as a welcoming and supportive environment to provide a service to students and the local community. It is meant to be utilized for their resources and provide a safe space where you are surrounded by people in an open and accepting space. Their core values include providing resources, sustainability, promoting diversity and inclusion, and helping members in the community community. The Canterbury House is not very recognized on campus, but they host a lot of events and activities, provide language lessons for international students, have a food pantry, have study and social spaces, and provide Wednesday night dinners such as the one I went to. Everyone I met there was very welcoming and insistent that I come back for following Wednesday night dinners. And I definitely want to. The environment created at the House is very comfortable. Their shared goal of creating an inclusive, diverse, welcoming, and supportive environment become more and more evident the more time I spent at the house. They aren’t the largest of groups, but they are a part of a social movement on campus.
I have seen a lot of the individuals I met that night throughout campus, in classes, in the library, or at other events. I learned a lot from going to the Canterbury house that night and hope to return and learn more. Their mission to create an inclusive campus is a beautiful one and I believe that with their influence and the help of others that it can be reached.
Sources:
https://www.involvement.mtu.edu/organization/canterbury-house-council
We often hear the saying “addiction does not discriminate” thrown around. It is an issue that is hard to relate it to a certain class, race, ethnicity, gender, sexuality, etc. Anyone can become addicted.
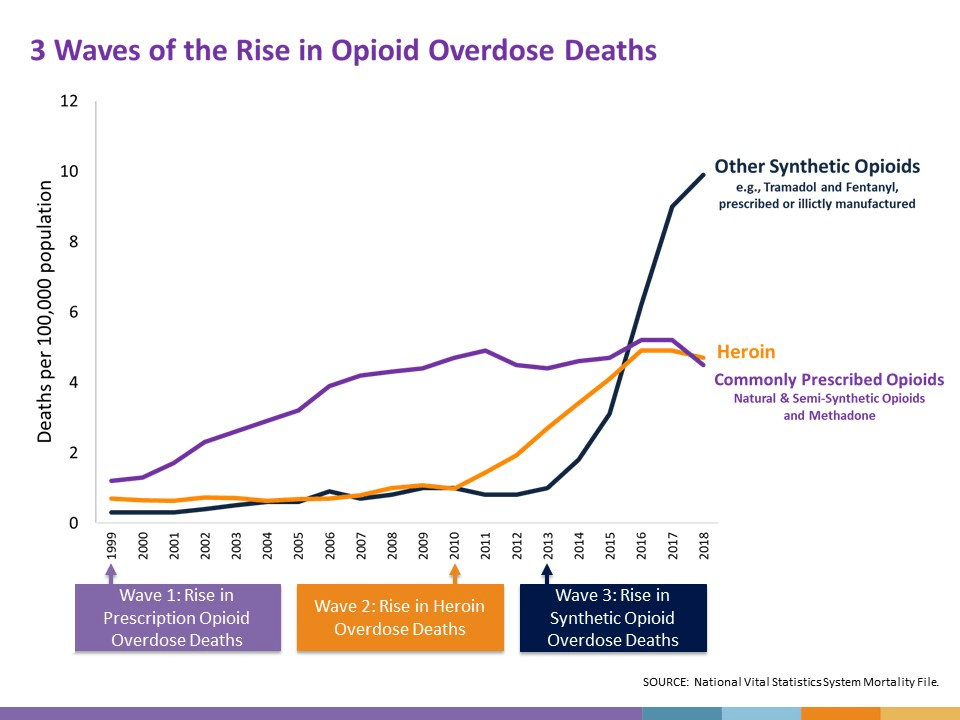
As seen in Understanding the Opioid Epidemic (a PBS documentary that traces the causes behind the growth in the use of prescription opioids and the impact they have in America), there are stories of people from all different backgrounds. It can start from being prescribed opioids from a sports injury, car accident, surgery, or something else. According to the documentary, “Health care providers wrote nearly a quarter of a billion opioid prescriptions in 2013. That is enough for every adult American to have their own bottle of pain pills. Anyone who takes prescription opioids can become addicted to them.” There has been a connection between the increase in the number of opioids prescribed, heroine dose deaths, and opioid overdose deaths in the recent years as you can see form the graph below.
The health care system as an institution holds a lot of power in causation and prevention as doctors may prescribe painkillers without thinking of the consequences. Stories in the documentary often start with medical treatment for moderate to severe pain that evolve into drug addiction which increases exponentially and may cause death. As a society, there has been an increase in the use and acceptance of prescription painkillers. Overdoses in America have been increasing among men and women of all races and ages. It affects nearly every area of the country and reaches into and impacts every neighborhood and socioeconomic group. According to the Centers for Disease Control and Prevention, “…every day approximately 91 people in the United States die from opioid overdose.” And the numbers those deaths and addictions affect are even greater and they are not just statistics. Understanding the Opioid Epidemic shows the impact of the overuse of prescription painkillers on individuals, families and communities.
Solutions to the opioid epidemic include improved opioid prescribing, reducing the amount prescribed and produced, and more non-drug treatment for pain. We need to prevent people from becoming addicted in the first place. And we need to better treat those that already addicted.
We are shown just how challenging fighting an addiction may be in Elaine McMillion Sheldon’s Recovery Boys (which follows four opioid addicts through their journey of recovery and sober living).
The film follows the ups and downs of their journey. Despite only focusing on a single demographic of straight, white males from the West Virginia, the stories of Jeff, Ryan, Rush, and Adam, show the struggles of someone seeking to escape the implications of addiction. The men cycle in and out of Jacob’s Ladder which is a farming-based rehab clinic that was founded by a specialist in critical care, Dr. Kevin Blankenship. Kevin acts as a father figure to the residents as they create a sober society of rehab at Jacob’s Ladder.
They spend their days working on a farm, caring for livestock, baling hay, farming for corn, and more. It adds structure to their lives when before they were uncertain and chaotic.
While in rehab, they have the structure and a societal support system from others that they did not have in the outside world. They make friends that help them stay accountable and remind them of why they are there. They build a supportive institution where they can share about their past and help build each other up. However, the effects of the rehab may not stay with them once they leave the six month program. Some enter back into the same cycle they were in before.
For example, once Jeff grad, a father of two young girls, graduates from the program and overdoses and relapses. After he is released from jail, he didn’t have a job (and as a 3 time felon it was very difficult to find one) or permission to leave his hometown. In the film his lawyer states how “It’s awful how they just let people be released, you know what I mean? I don’t know how people are supposed to get a good footing and follow the rules of probation when they don’t have any resources…” Jeff’s situation continued to create a division and perpetuate and inequality in his life. He was thrown back into a community where the social influences were negative and impacted him very differently from the supportive and structured program at Jacob’s Ladder. In his hometown he spends time with his addicted relatives and friends and shows how steep the pathway to sobriety can be as he once again gets stuck in a cycle of addiction.
In the end it is up to the addict to decide whether to live sober or not. Each case in Recovery Boys was unique, but the latter is true. Some reap the benefits of recovery, but not everyone can finish the process. The bond between the men in the program became very important in that decision as they help and influence each other through accountability, open self-reflection, and a certain level of intimacy while sharing. When one would begin falling back into old habits they would mutually show their support and love as they openly cried and spoke about their hardships and worries. This is rare for these men in the communities they grew up with in the South.
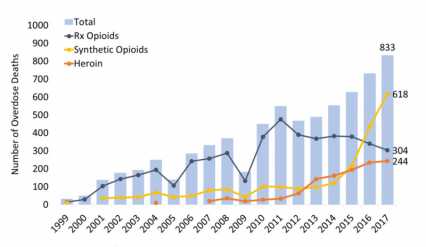
When you dive deeper into the issue of addiction, you can see that it affects some more than others. Recovery Boys takes place in West Virginia which is the heart of America’s opioid epidemic. West Virginia has the highest drug overdose death rate in the United States. You can see some of the statistics of it growing in the figure below. In the film, one of the residents describes the influence a society can have on a person and how it was inevitable he became a drug addict, “drugs and alcohol, that’s what I grew up around… I thought that was just how everybody lived. I didn’t know people lived life sober.” This way of life may be the result of factors such as high rates of unemployment in West Virginia and a high number of jobs involving manual labor such as coal mining, timbering, and manufacturing. For a long time, West Virginia has been known as “coal country.” These are jobs that require heavy manual labor and may leave their workers prone to injury.
This cycles us back to the beginning of my post, of why opioids are prescribed in the first place. Opioids are legally prescribed, which may lead to addiction, which may lead overdosing or acquiring cheaper drugs such as heroine and starts this cycle of addiction that is very difficult to overcome. Understanding the Opioid Epidemic and Recovery Boys show how this cycle is created using sounds evidence and stories from individuals. Even though we hear the phrase, “addiction doesn’t discriminate,” we can still see the inequalities it creates as those affected become stuck in a cycle. These films are not the best for students seeking to understand inequality as it can affect anyone and that it shown over and over again from the stories we hear. However, the films are powerful in showing the power of our health care system and the exponential negative effects of something that started off as a helpful action.
Sources:
“Heroin(e) and Recovery Boy Films.” Heroin(e) and Recovery Boy Films, recoveryboysthefilm.com/.
Jacobs, Harrison. “Here’s Why the Opioid Epidemic Is so Bad in West Virginia – the State with the Highest Overdose Rate in the US.” Business Insider, Business Insider, 1 May 2016, http://www.businessinsider.com/why-the-opioid-epidemic-is-so-bad-in-west-virginia-2016-4.
National Institute on Drug Abuse. “West Virginia Opioid Summary.” NIDA, 29 Mar. 2019, http://www.drugabuse.gov/opioid-summaries-by-state/west-virginia-opioid-summary.
“PBS.” PBS, Public Broadcasting Service, http://www.pbs.org/show/understanding-opioid-epidemic/.
“Understanding the Epidemic.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 19 Mar. 2020, http://www.cdc.gov/drugoverdose/epidemic/index.html.
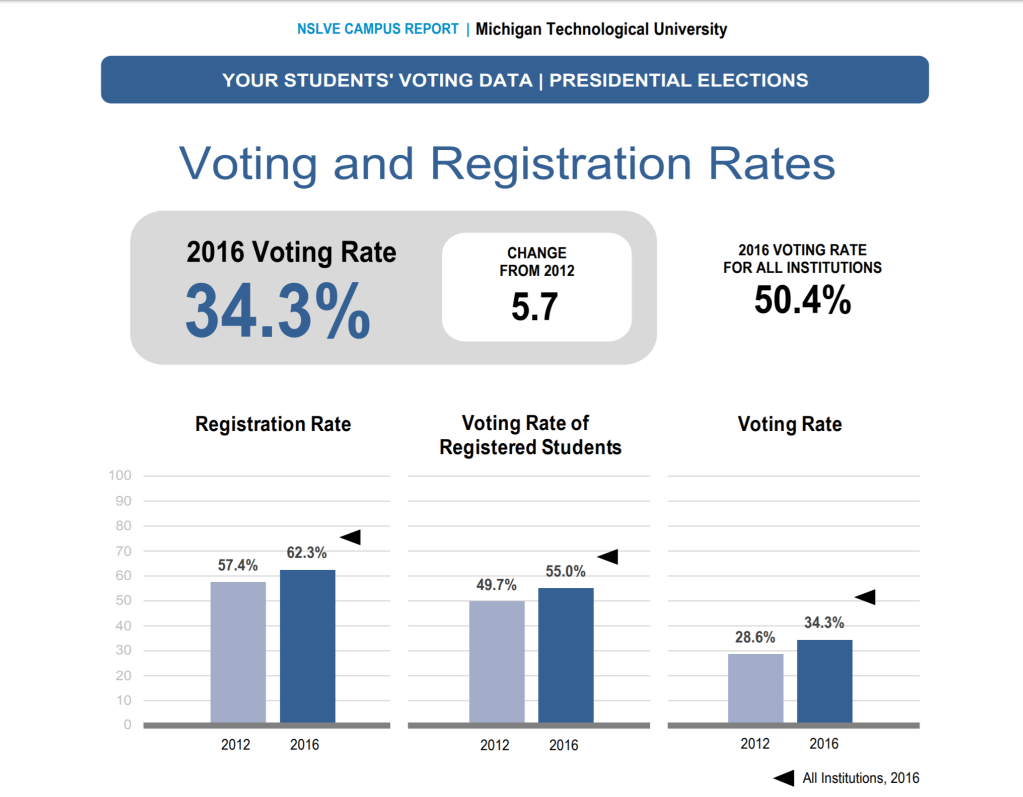
Since the United States of America consists of a Representative Democracy, voting is an important form of civic engagement in our democratic society. However, approximately only 56% of the voting age population in the United States participates according to an NSLVE study. Statistically, older people vote at a much higher rate than the younger population does. Compared to Universities at a national level, Michigan Technological University voter participation is well below the average as you can see in the image below. Even after in increase in voter participation since the 2012 election, Michigan Tech still only had a 34.3% voting rate in the 2016 election. The voting rate for other institutions was around 50.4%. Both registration and voting rates at Michigan Tech are much lower than other institutions.
This may be caused by differences in the social norms at Michigan Tech. Michigan Tech culture is unlike a lot of other universities. Michigan Tech is not a liberal arts college, but instead focused and invested in mechanics and technology instead of the social environment that we live in or are trying to live in. Students aren’t as aware of the elections as they focus more on their schoolwork rather than politics. Michigan Tech lacks the resources to advocate for students to vote. When I walk around campus, I am not faced with “Please vote!” or “Don’t forget to vote!” signs posted everywhere I look. In fact, it is rare I see any information encouraging students to vote, why to vote, or how to vote. There are very little to none posters, emails, or political clubs on campus. Voting is not highly encouraged on Tech’s campus and the topic of upcoming elections is rarely brought up. For example, the first time I heard about the primary election coming up was in my Intro to Sociology class. We have an election in less than a week and I hadn’t even heard about it!

One way to help solve this issue is to start doing more as a university to advocate for student votes. Clubs could set up booths in the library to let students know about the upcoming election. Posters could be displayed in Fisher. Pamphlets can be placed on the dining hall tables. The administration could send out an email to encourage students to vote and giving information on how to vote without directing who to vote for. Professors could mention the election in classes amd remind students to vote. Individuals or clubs can work to put out propaganda from multiple media platforms to spread information and awareness for the upcoming elections. We need to work on making information about the election visible to students on campus. This is needed to socialize students into thinking that voting is normal and that this is what we are supposed to do. We need to work on creating into a social norm.
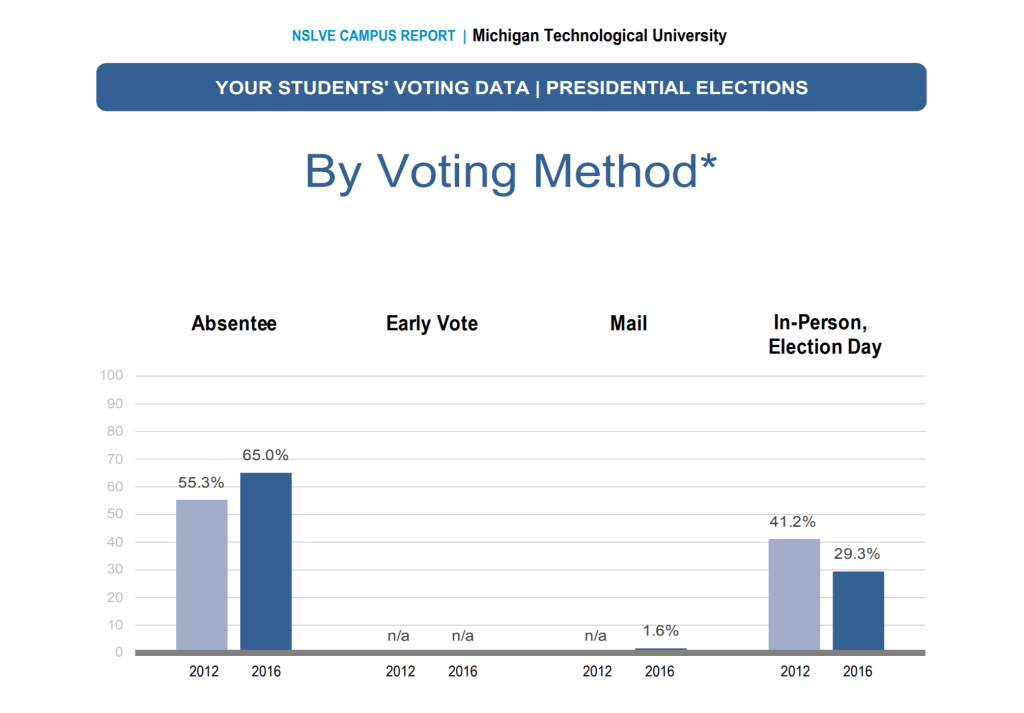
MTU student voter participation rates may be so much lower than the national average across participating students in the NSLVE study because of the rural location of our campus. The majority of Michigan Tech students vote absentee. As you can see in the image below, in the 2016 election, 65% of Michigan students voted by absentee method compared to only 29.3% in person.
The difficulty for students to vote may play a huge role. Many college students want to keep their home address, but don’t have enough time to go home to register to vote or to vote at the resident address on their driver’s license. Most Michigan Tech students live over 8 hours away, while the average distance away from home for other universities is only about 2 to 3 hours. Students also may not have voted because they didn’t want to vote absentee due to the old laws that required a lot of additional work. You used to have to physically hand your absentee ballot to the clerk to vote absentee for your first time in Michigan. You were also required to request your absentee ballot 45 days ahead of the election. Most students don’t even have the election on their radar at that point in time. After that process, the absentee ballot still had to come to the right address instead of your home address.
However, laws were changed in 2016 to make voting easier. You can now register to vote up until the day of an election. You can register to vote online. You can request absentee ballots up until the election date. This may have a big impact on the amount of student that vote in this year’s election.
Another policy that has been proposed to help in the voting process is to default register everyone to vote when they get their drivers license unless they choose to opt out. Registration rates at Michigan Tech are already higher than our voting rates and increasing, but still short of national average for institutions. This method will greatly increase the number of students that are registered to vote.
Another method that would help with the ease of voting (if it were allowed) would be to have a place on campus where you could register to vote before the election and even a place on campus to vote on election day. If we could have an on-campus place to vote, we would see a significant increase in voting rates as it would be seen as a norm in our institution. Another option that is easier to implement would be a shuttle running from campus to the polls throughout the day. As the ease of getting to the polls increases, it should lead to an increase in voting rates.
There are many methods we can implement in hope that the voting rates at Michigan Tech increase. After the proposals that went into effect after the 2016 election, it is now way easier for college students to vote in Michigan than before. We need to work to add voting as a normality at Michigan Tech. As of right now, millions of people don’t have a voice. This perpetuates inequalities and further concentrated power as the whole election process will become run by just the few people that have a real interest. This may not be the best for the majority of people. We need to work to spread awareness on campus in order to get students involved and to participate. We need this for our democracy to function.
NSLVE: Student Voting Rates for Michigan Technological University
“Why are you so beautiful?”… “That’s the way God made me,” I would giggle.
“Why are you so smart?”… “That’s the way God made me,” I would reply.
This was the response I was taught to give to any question my dad asked of me.
Those I surrounded myself with and my past experiences have transformed me into the role of a missionary. Not in the ordinary sense where a missionary travels the world sharing the good news of our Lord. I would classify myself as a missionary in my own backyard. This is shown to others through my actions and words as I help pass what I have learned throughout my life.
Intergenerational experiences are not as central to our lives as they once were. However, growing up, I spent a lot of time as my mom’s helper. I would go to the nursing homes with her and build puzzles and talk with the residents as she finished her rounds. Through their stories, I learned great lessons for as Job 12:12 says, “Is not wisdom found among the aged? Does not long life bring understanding?” Believing in this teaching, my family spent a lot of time visiting the elders in my church and neighborhood.
In first grade, we were told to draw a picture of ourselves at one-hundred years old. Mine was radically different and I soon realized that I was socialized in a very different way as my peers. I spent more time with elders than friends my own age. While my friends drew themselves as old ladies with white hair, walking their dogs, I drew myself an old lady, missing teeth, in a wheelchair, children climbing all over, with four angels looking down at me from heaven. Reflecting on this picture now, I realize this old lady lived her life to the fullest. She had adventures, imparted her wisdom on children, and knew where she was going and where she had come from. I realized she was very similar to the neighbor that I spent the majority of my time learning from — Beegu.
Beegu (Finnish for little girl) is an affectionate nickname for an old lady who lives on a small farm down the hill from mine, in what is known as “The Valley.” Imagine a little cottage, somewhat styled like a house in a children’s bedtime story, very small and cozy, with over a dozen unwinded cuckoo clocks that go off whenever they please because there she insists the concept of time is nonlinear. Here, time is a series of moments—teaching moments about prayer, God, and the importance of sharing our faith with family and one another. There is no question that blue is her favorite color, as it is the tone of everything, down to the wooden trim on her house, the boiling kettle, and her blue woodstove. Her doors are always open, and I along with the other children in “The Valley” are frequent visitors. She calls us her “Gorgeous Meatballs” and never misses a chance to share stories from her past and impart her wisdom on the generations to come. She has led me and many other “Valley kids,” to understand true discipleship is about keeping God centered in our lives—through prayer and serving others. She is the sounding board for all of us as we try to discern our calling. All the “Valley kids” learned many lessons from Beegu that affect our mannerisms. We learned how to treat others. We learned to thank the Lord for what He provides us. We learned to pray for ourselves and others. We learned to memorize bible verses, poems, and songs. Together, us “Valley kids” became socialized in a very different way than our other friends. The norms when at Beegu’s were very different from how others acted elsewhere. But she taught us not to change who we are when in the community. She gave us a new set of values and reinforced them into our lives. She taught us how to share this with others so we could become missionaries among our friends. She taught us how to become missionaries in our own backyard.
Because of the people I surrounded myself with, the influences I had growing up, the expectation for me to go to church, and the constant reminder from my mother to “Stop being sacrilegious” or to “pray about it” when I had an issue, I learned to keep God central in my life at all times. If I hadn’t spent as much time at Beegu’s house growing up or with the other “Valley kids” I would have been socialized in a different way. I may even have completely different beliefs. I may act in very different ways. But because of my experiences, I am comfortable with keeping God first throughout life as my faith gives me direction and sets my moral compass.
The implications of this socialization for my life today have made a huge impact on my life and impacts many of my life choices. It helps me live my life to the fullest just like the old lady from my drawing in first grade as I know where I come from and now am learning where to go. I like to think of myself as a missionary as it is the way I was raised. It is what is expected of me.
I appreciate other people’s beliefs and respect them. We were all socialized in different ways and that socialization makes a huge impact on different aspects of our life including faith. However, I believe that through my love and support for others I can help enhance other’s lives through my actions. We can learn from each other and the effects of our socialization on our beliefs. My role is difficult as I know not everyone has the same beliefs as mine and I am okay with that. Even though my beliefs may challenge others, I still have an open mind to learning and modify my own beliefs when I hear input from other people. Throughout life, we are always learning from each other. It is amazing to see how the differences in the ways we are socialized can affect our lives. I have fallen into my societal roles because of the people I grew up with and the way I was socialized. One of those roles I identify myself in is being a missionary.
This is an example post, originally published as part of Blogging University. Enroll in one of our ten programs, and start your blog right.
You’re going to publish a post today. Don’t worry about how your blog looks. Don’t worry if you haven’t given it a name yet, or you’re feeling overwhelmed. Just click the “New Post” button, and tell us why you’re here.
Why do this?
The post can be short or long, a personal intro to your life or a bloggy mission statement, a manifesto for the future or a simple outline of your the types of things you hope to publish.
To help you get started, here are a few questions:
You’re not locked into any of this; one of the wonderful things about blogs is how they constantly evolve as we learn, grow, and interact with one another — but it’s good to know where and why you started, and articulating your goals may just give you a few other post ideas.
Can’t think how to get started? Just write the first thing that pops into your head. Anne Lamott, author of a book on writing we love, says that you need to give yourself permission to write a “crappy first draft”. Anne makes a great point — just start writing, and worry about editing it later.
When you’re ready to publish, give your post three to five tags that describe your blog’s focus — writing, photography, fiction, parenting, food, cars, movies, sports, whatever. These tags will help others who care about your topics find you in the Reader. Make sure one of the tags is “zerotohero,” so other new bloggers can find you, too.
